Tumour necrosis factor α, IL-23 and IL-17A are key targets for psoriasis therapy based on an understanding of the key role that these cytokines play in the pathophysiology of disease.
Highly encouraging results have been found for several new agents that target these mechanisms.
Psoriasis is a chronic, immune-mediated disease with a complex pathogenetic process triggered by a combination of genetic and environmental factors that induce secretion of tumour necrosis factor (TNF) α by keratinocytes, which in turn activates dendritic cells. There are various limitations associated with existing therapies, although new understanding of the pathogenesis of psoriasis has led to the development of novel targeted therapeutics. Interleukin inhibitors represent a major therapeutic advance, as they appear to be highly selective in terms of mitigating the perturbed inflammatory pathways responsible for psoriasis.
The IL-23/IL-17 pathway is a critical axis in the pathogenesis of psoriasis, and IL-17A is the primary effector. Indeed, IL-17A overexpression is a defining feature of plaque psoriasis. [1]
Secukinumab and ixekizumab are monoclonal antibodies to IL-17A, while brodalumab is a monoclonal antibody targeting IL-17RA.
Clinically, IL-17 antagonists have demonstrated good efficacy, long-term maintenance of treatment response and a quick onset of action. [1]
The unprecedented efficacy of these agents further supports that the pathogenesis of psoriasis is largely driven by the Th17 axis.
Importantly, these biologic agents represent additional therapeutic modalities in individuals who are eligible for systemic therapies.
IL-1 and IL-36 are the highly expressed dominant cytokines in generalised pustular psoriasis. In comparison, the expression of IL-17 and IL-22 is reduced. [2]
Anakinra is a synthetic, injectable, IL-1 receptor antagonist that has led to exciting results in pustular psoriasis in patients with no response to anti-TNF agents.
Inhibition of the IL-36 pathway has also been recently examined in pustular psoriasis. [3]
In particular, a phase I proof-of-concept study has been performed in 7 patients who presented with a generalised pustular psoriasis flare and treated with a single, open-label, intravenous dose of BI 655130, a monoclonal antibody against the IL-36 receptor. [4]
Pustules were completely cleared in three patients within 48 hours after treatment, in 5 patients by week 1 and in 6 patients by week 2.
The results were maintained until at least 20 weeks when the study ended.
Thus, blockade of both the IL-1 and IL-36 pathways is associated with extremely good clinical response, consistent with the observed overexpression of the two cytokines.
In other forms of psoriasis, the IFN pathway appears to be involved in pathogenesis. [4]
Indeed, in animal models, blocking signaling of IFN-α or inhibiting the ability of plasmacytoid predendritic cells (PDC) to produce IFN-α prevented T cell-dependent development of psoriasis.
This suggests that PDC-derived IFN-α represent a potential early target for the treatment of psoriasis.
Future strategies to target PDCs in psoriasis include those aimed at IFN blockade: anti-IFN-α (sifalimumab); anti-IFN receptor (anifrolumab); the TYK2 inhibitor BMS-986165.
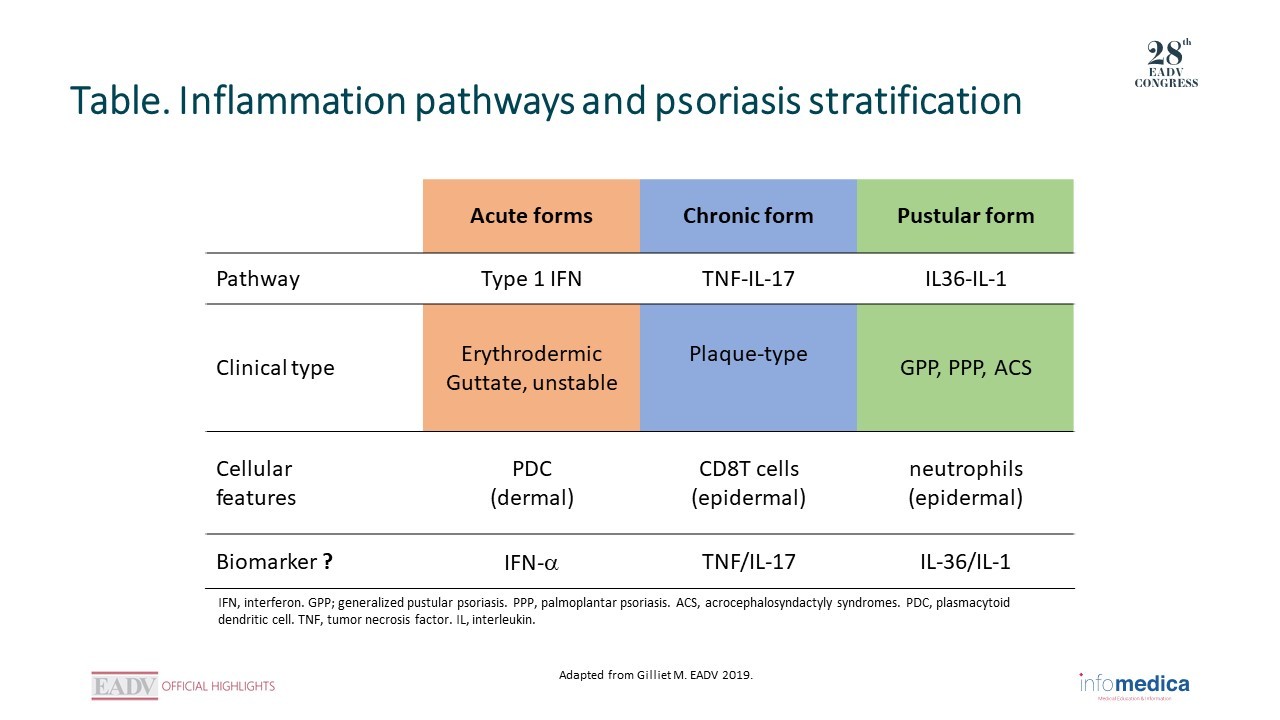
Given the increased understanding of the inflammatory pathways at the basis of the different types of psoriasis, a basic stratification scheme can be proposed (Table).
For the acute forms (such as the erythrodermic, guttate and unstable forms), type I IFN is involved.
TNF-IL-17 is involved in the chronic plaque-type forms, and IL-1/IL-36 in the pustular forms.
Based on this knowledge, it is becoming clearer that therapeutic blockade of the appropriate target can be very effective clinically.
Bachelez H, Choon SE, Marrakchi S, et al. Inhibition of the interleukin-36 pathway for the treatment of generalized pustular psoriasis. N Engl J Med. 2019 Mar 7;380(10):981-3.
Gilliet M, Conrad C, Geiges M, et al. Psoriasis triggered by toll-like receptor 7 agonist imiquimod in the presence of dermal plasmacytoid dendritic cell precursors. Arch Dermatol. 2004 Dec;140(12):1490-5.
Presenter disclosure information: M Gilliet: Abbvie, Amgen, Celgen, Galderma, Genentech, La Roche-Posay, Lilly, Novartis, Roche.
Presented by: Prof. Kristian Reich, Translational Research in Inflammatory Skin Diseases, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, and Skinflammation® Center, Hamburg, Germany
Presented by: Prof. Spyridon Gkalpakiotis, Department of Dermatovenereology, Third Faculty of Medicine and University Hospital of Kralovske Vinohrady, Prague, Czech Republic.
 RATE THIS PROGRAM
RATE THIS PROGRAM

 Deutsch
Deutsch Español
Español Français
Français Italiano
Italiano Português
Português יהודי
יהודי