24-week results from a multicentre, randomised study evaluating ixekizumab versus adalimumab in psoriatic arthritis patients with psoriasis of ≥10% or <10% body surface area involvement at baseline
Presented by:
Prof. Saxon Smith
Dermatology Centre, Hospital CUF Descobertas, Lisbon, Portugal
In bDMARD-naïve patients with PsA and concomitant PsO, ixekizumab was associated with greater response than adalimumab on skin and joint outcomes, independently of baseline body surface area.
The selective interleukin-17A inhibitor ixekizumab (IXE) is approved for the treatment of active psoriatic arthritis (PsA) and moderate-to-severe plaque psoriasis (PsO). The SPIRIT-H2H study evaluated the efficacy and safety of IXE versus adalimumab (ADA), another biologic disease-modifying antirheumatic drug (bDMARD), approved in patients with PsA and PsO. [1]
This post-hoc subgroup analysis evaluated various 24-week efficacy outcomes from SPIRIT-H2H in patients with high or low PsO body surface area (BSA) involvement at baseline.
SPIRIT-H2H was a multicentre, open-label, rater-blinded, parallel-group study in which bDMARD-naïve patients (N=566) with PsA and active PsO (≥3% BSA involvement) were randomised to IXE or ADA for 52 weeks.
Dosing was based on the baseline severity of PsO:
Moderate-to-severe PsO was defined as PASI score ≥12, sPGA ≥3 and BSA involvement ≥10%.
Patients with moderate-to-severe PsO received:
IXE (160 mg at week 0, 80 mg Q2W up to week 12 then Q4W). or
ADA (80 mg at week 0, 40 mg Q2W starting at week 1).
Patients not fulfilling the criteria for moderate-to-severe PsO received:
IXE (160 mg at week 0, 80 mg Q4W), or
ADA (40 mg at week 0, 40 mg Q2W),
Primary outcome measure
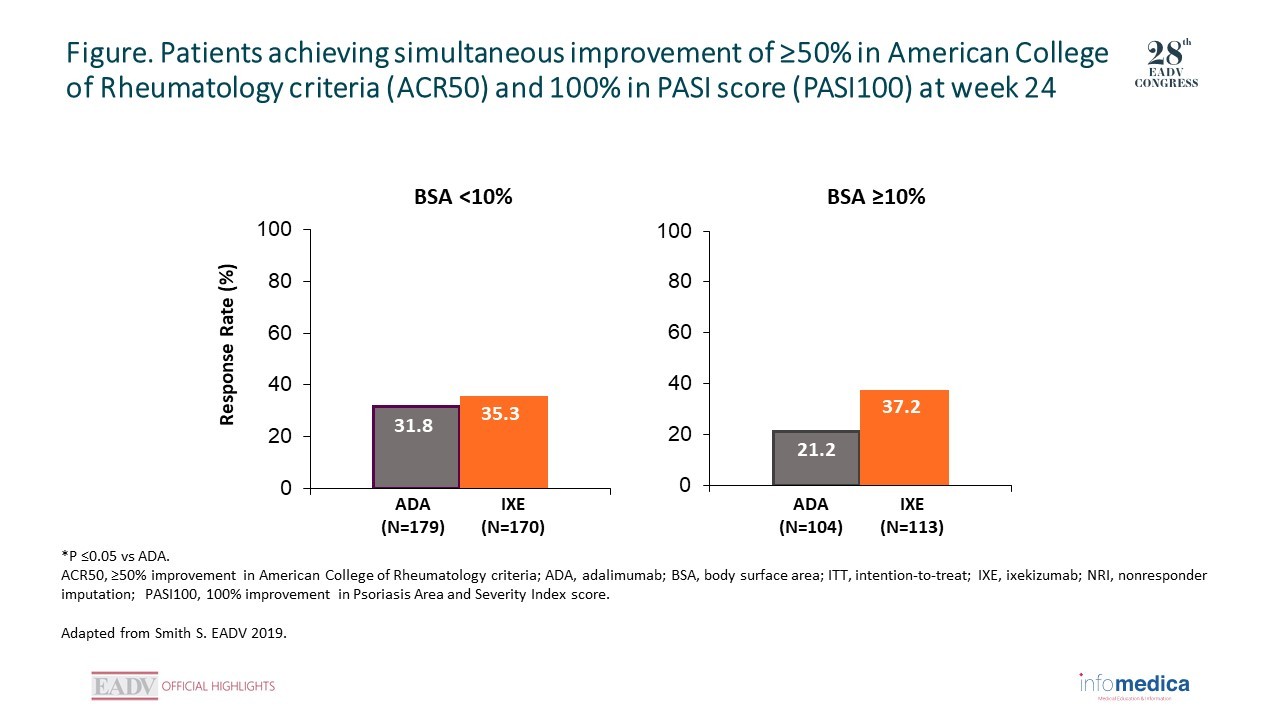
The primary endpoint was the proportion of patients achieving simultaneous improvement of ≥50% in American College of Rheumatology criteria (ACR50) and 100% in PASI score (PASI100) at week 24.
In this post-hoc subgroup analysis, efficacy outcomes at week 24 were compared between IXE and ADA in patients with baseline BSA involvement of ≥10% or <10%.
At baseline, patients with BSA ≥10% (n=217) consistently showed higher arthritis- and skin-related clinical assessment scores, and worse patient-reported outcomes, than patients with BSA <10% (n=349).
With regards to the simultaneous achievement of ACR50 and PASI100 at week 24, consistent response rates across baseline BSA levels were observed among IXE-treated patients (37.2%, and 35.3% for high and low BSA, respectively) (Figure).
Among ADA-treated patients, a lower response rate was observed in the high compared to the low BSA subgroup (21.2% vs 31.8%), resulting in a significant difference versus IXE.
PASI100 and PASI90 responses were significantly higher for IXE than ADA in both subgroups.
By contrast, PASI75 responses were significantly higher for IXE only in the subgroup with BSA <10%.
For ACR50, responses were similar for IXE versus ADA in both subgroups. Remission rates based on Disease Activity in Psoriatic Arthritis scores and Minimal Disease Activity (MDA6) were significantly higher for IXE than ADA in the BSA ≥10% subgroup.
Dermatology Life Quality Index (0,1) responses were also significantly higher for IXE than ADA in the BSA ≥10% subgroup.
IXE was associated with higher levels of response than ADA for skin and joint outcomes in bDMARD-naïve patients with active PsA and concomitant PsO, regardless of BSA involvement at baseline.
For patients with ≥10% BSA involvement, IXE was associated with a statistically significant better efficacy outcome than ADA with respect to the primary endpoint.
Data from this post-hoc analysis are consistent with the findings of the SPIRIT-H2H study.
Key messages/Clinical perspectives
In bDMARD-naïve patients with PsA and concomitant PsO, IXE was associated with higher levels of response than ADA on skin and joint outcomes, irrespective of baseline BSA involvement.
Mease PJ, Smolen JS, Behrens F, et al. A head-to-head comparison of the efficacy and safety of ixekizumab and adalimumab in biological-naïve patients with active psoriatic arthritis: 24-week results of a randomised, open-label, blinded-assessor trial. Ann Rheum Dis. 2019 Sep 28. pii: annrheumdis-2019-215386.
Presenter disclosure information: S Smith: AbbVie, BMS, Eli Lilly and Company, Janssen-Cilag, Leo Pharma, and Novartis, Sanofi Genzyme.
Presented by: Prof. Kristian Reich, Translational Research in Inflammatory Skin Diseases, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, and Skinflammation® Center, Hamburg, Germany
Presented by: Prof. Spyridon Gkalpakiotis, Department of Dermatovenereology, Third Faculty of Medicine and University Hospital of Kralovske Vinohrady, Prague, Czech Republic.
 RATE THIS PROGRAM
RATE THIS PROGRAM

 Deutsch
Deutsch Español
Español Français
Français Italiano
Italiano Português
Português יהודי
יהודי