Efficacy and safety of ixekizumab in a phase 3, randomized, double-blind, placebo-controlled study in paediatric patients with moderate-to-severe plaque psoriasis
Presented by:
Prof. Kim A. Papp
Department of Medicine, Division of Dermatology, University of Toronto, Toronto, Canada
In paediatric patients with moderate-to-severe plaque psoriasis, ixekizumab was superior to placebo in improving skin, itch and health-related quality of life, with no unexpected safety findings.
Ixekizumab (IXE) is a high-affinity monoclonal antibody that selectively targets interleukin-17A, and which has been approved for treatment of moderate-to-severe plaque psoriasis in adult patients. [1] There is an unmet medical need for effective and safe therapies for children and adolescents with moderate-to-severe plaque psoriasis.
This randomised, double-blind phase III study (NCT03073200) evaluated the efficacy and safety of IXE in paediatric patients with moderate-to-severe plaque psoriasis.
Patients (6 to <18 years of age) with moderate-to-severe plaque psoriasis (Psoriasis Area and Severity Index (PASI) ≥12, static Physician’s Global Assessment (sPGA) ≥3, and body surface area involvement ≥10%) were randomised (2:1) to IXE every 4 weeks (Q4W) (N=115) or placebo (PBO) (N=56).
Patients randomised to IXE received 40 mg (<25 kg), 80 mg (25 to 50 kg), or 160 mg (>50 kg) starting doses (based on body weight), then 20 mg, 40 mg, or 80 mg (respectively) IXE Q4W through week 12
An active reference arm, etanercept (ETN), was also used.
Primary outcome measure
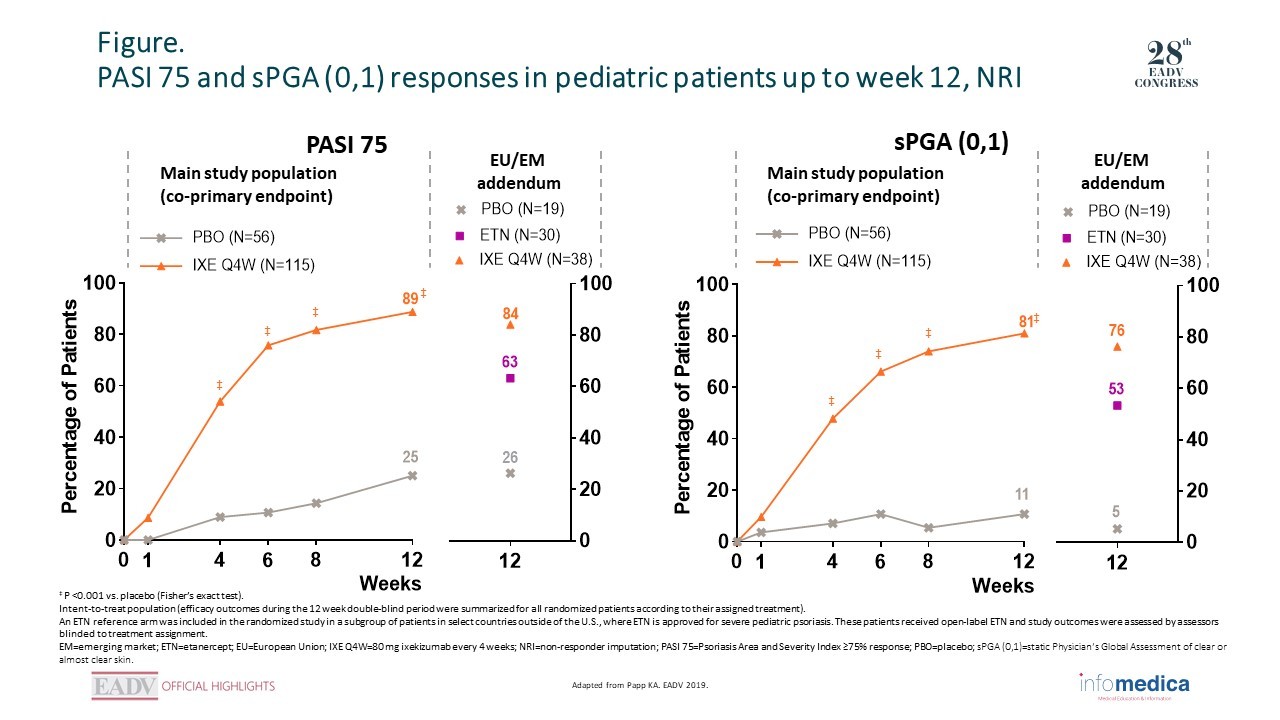
Co-primary endpoints were the proportion of patients achieving 75% improvement from baseline in PASI (PASI 75) and sPGA of clear or almost clear skin (sPGA 0,1) at week 12.
Overall, 98% (IXE), 97% (ETN) and 95% (PBO) of patients completed week 12 assessments; thus, the co-primary endpoints were achieved.
At week 12, IXE was superior to PBO for PASI 75/90/100 (IXE: 89%/78%/50%, PBO: 25%/5%/2%, P <0.001), sPGA 0,1 (IXE: 81%, PBO: 11%, P <0.001) and sPGA 0 (IXE: 52%, PBO: 2%, P <0.001) responses. At week 4, IXE was superior to PBO for PASI 75 (IXE: 54%, PBO: 9%, P <0.001) and sPGA 0,1 (IXE: 46%, PBO: 6%, P <0.001) (Figure).
IXE resulted in significantly (P <0.001) greater responses at week 12 for both Itch NRS ≥4 (IXE: 71%, PBO: 20%) and CLDQI/DLQI 0,1 (IXE: 64%, PBO: 23%).
Among patients receiving ETN, PASI 75/90/100 responses were 63%/40%/17%; sPGA (0,1) response was 53%; and sPGA (0) response was 17%.
Treatment-emergent adverse events (TEAEs) occurred in 45% (PBO) and 56% (IXE) of patients; none were severe.
The most common TEAEs in the IXE group (occurring in ≥10% of IXE-treated patients) were nasopharyngitis (11.3%) and headache (10.4%).
Significantly more patients treated with ixekizumab versus placebo achieved PASI 75 and sPGA (0,1) as early as week 4.
Most adverse events were mild or moderate in severity and the safety profile was generally consistent with that seen in adults with moderate-to-severe plaque psoriasis.
Key messages/Clinical perspectives
IXE was superior to PBO in improving skin, itch and health-related quality of life in paediatric patients with moderate-to-severe plaque psoriasis, with no unexpected safety findings.
Liu L, Lu J, Allan BW, et al. Generation and characterization of ixekizumab, a humanized monoclonal antibody that neutralizes interleukin-17A. J Inflamm Res. 2016 Apr 19;9:39-50.
Presented by: Prof. Kristian Reich, Translational Research in Inflammatory Skin Diseases, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, and Skinflammation® Center, Hamburg, Germany
Presented by: Prof. Spyridon Gkalpakiotis, Department of Dermatovenereology, Third Faculty of Medicine and University Hospital of Kralovske Vinohrady, Prague, Czech Republic.
 RATE THIS PROGRAM
RATE THIS PROGRAM

 Deutsch
Deutsch Español
Español Français
Français Italiano
Italiano Português
Português יהודי
יהודי