Prurigo nodularis (PN) is a subtype of chronic prurigo that is highly pruritic, chronic, difficult to treat and associated with high disease burden. [1] The pathogenesis of PN is not completely understood, although inflammatory pathways have strongly implicated the involvement of IL-31. [2] Nemolizumab is a humanised monoclonal antibody targeting the IL-31 receptor alpha subunit that is under development for treatment of severe pruritic skin diseases.
Multicentre (20 sites, EU), randomised, double-blinded, placebo-controlled, parallel group study.
Patients had to have had a clinical diagnosis of PN for at least 6 months, with least 20 nodules on the body with bilateral distribution and severe pruritus (NRS (Numerical Rating Scale) ≥7).
A total of 70 patients were randomised to placebo (N=36) or nemolizumab (N=34).
Primary outcome measure
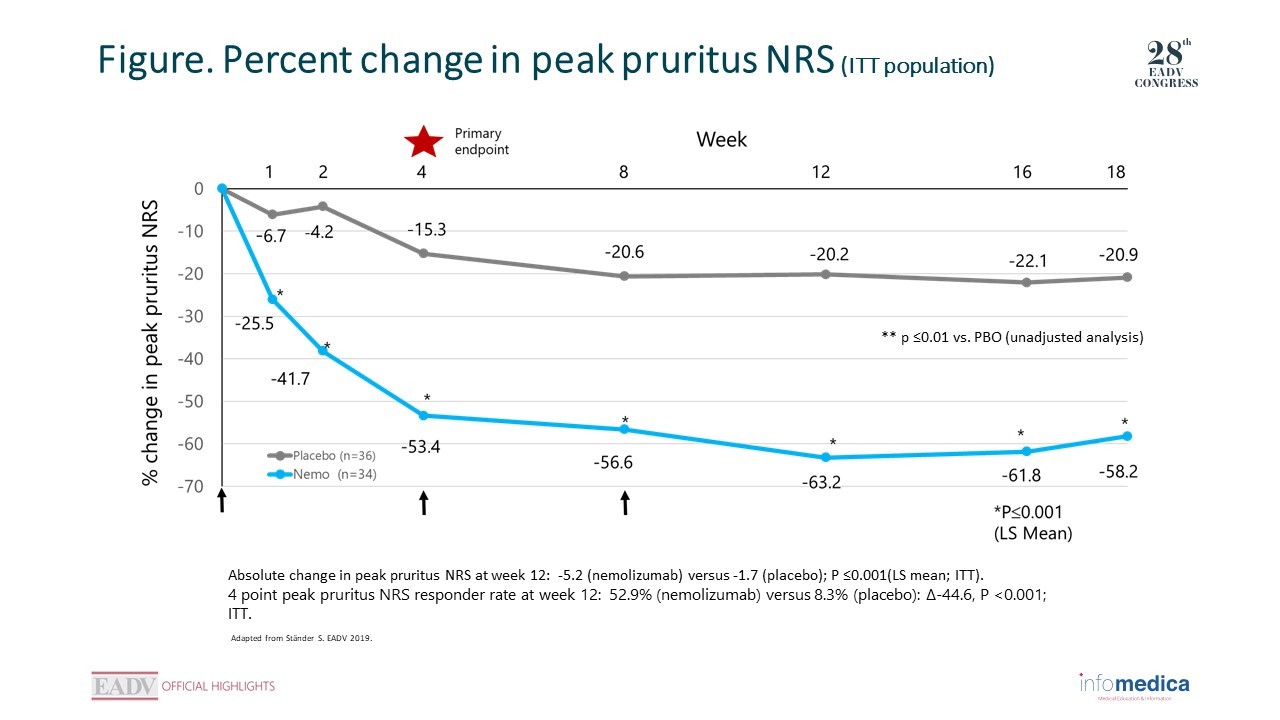
The primary endpoint was percent reduction from baseline in peak pruritus NRS at week 4.
Overall, baseline characteristics were similar between groups.
Changes in the primary endpoint, percent change in peak pruritus NRS, were significant within week 1 and remained significant at all time points thereafter.
The absolute change in peak pruritus NRS at week 12 was-5.2 for nemolizumab vs -1.7 for placebo; P ≤0.001.
4-point peak pruritus NRS responder rate at week 12 was 52.9% for nemolizumab vs 8.3% for placebo: Δ-44.6, P <0.001; ITT (Figure).
There was no difference in peak pruritus between patients with and without atopic predisposition.
At week 18, significantly more patients reached IGA success with nemolizumab (44.1% than with placebo (5.6%; P = 0.001).
At week 18, significantly more patients achieved PASI75 with nemolizumab (38.2% than with placebo (8.4%; P <0.001).
Nemolizumab was also associated with significant improvement in sleep disturbance from baseline vs placebo.
In the nemolizumab group 5.9% of patients discontinued the study medication for an adverse event vs 5.6% for placebo.
Overall, the adverse event profile was similar between groups.
Nemolizumab resulted in a rapid and clinically relevant improvement of pruritus and nodular lesions in PN with onset of effect on pruritus as early as week 1 with 38% of patients clear or almost clear of skin lesions.
Nemolizumab was significantly more effective than placebo in all clinical endpoints
Nemolizumab was well tolerated with a similar safety profile vs placebo.
Key messages/Clinical perspectives
Nemolizumab demonstrated highly encouraging results compared to placebo in treatment of PN in phase II trials, warranting additional studies.
Presenter disclosure information: S Ständer: has received research funds from DFG, EADV, BMBF, and IZKF and has served as a consultant for Almirall, Bayer, Beiersdorf, Bellus Health, Bionorica, Cara Therapeutics, Celgene, DS Biopharma, Galderma, Kneipp, Maruho, Menlo Therapeutics, Marz, NeRRe Therapeutics, Novartis, Nuformix, Perrigo, Sienna Therapeutics, ACO HUD Nordic, Toray, Trevi Therapeutics and as an investigator for Dermasence, Galderma, Kiniksa, Menlo Therapeutics, Trevi Therapeutics, Novartis, Sanofi, Vanda Therapeutics.
Presented by: Prof. Kristian Reich, Translational Research in Inflammatory Skin Diseases, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, and Skinflammation® Center, Hamburg, Germany
Presented by: Prof. Spyridon Gkalpakiotis, Department of Dermatovenereology, Third Faculty of Medicine and University Hospital of Kralovske Vinohrady, Prague, Czech Republic.
 RATE THIS PROGRAM
RATE THIS PROGRAM

 Deutsch
Deutsch Español
Español Français
Français Italiano
Italiano Português
Português יהודי
יהודי