Vitiligo is a chronic autoimmune disease that targets melanocytes, resulting in patches of skin depigmentation. [1] The pathogenesis of vitiligo is driven by signalling through JAK1/JAK23, and a cream formulation of ruxolitinib, a JAK1/JAK2 inhibitor, [2] is under investigation for the treatment of the condition. [3] Ruxolitinib cream provided significant repigmentation of facial vitiligo lesions after 24 weeks of double-blind, vehicle-controlled treatment (NCT03099304). [4]
Trial NCT03099304 was a randomised, double-blind, dose-ranging study of ruxolitinib phosphate cream in subjects with vitiligo.
Patients had to have a clinical diagnosis of vitiligo with depigmented areas including ≥0.5% of total Body Surface Area (BSA) on the face and ≥3% of total BSA on non-facial areas.
Patients in the previous groups (0.5% QD, 1.5% QD, 1.5% BID) of trial NCT03099304 continued treatment.
Subjects on vehicle and those in the 0.15% group were rerandomised if <25% improvement in facial Vitiligo Area Scoring Index (F-VASI) was seen at week 24.
Re-randomisation was to 0.5% QD, 1.5% QD, or 1.5% BID.
A total of 157 patients were studied.
Primary outcome measure
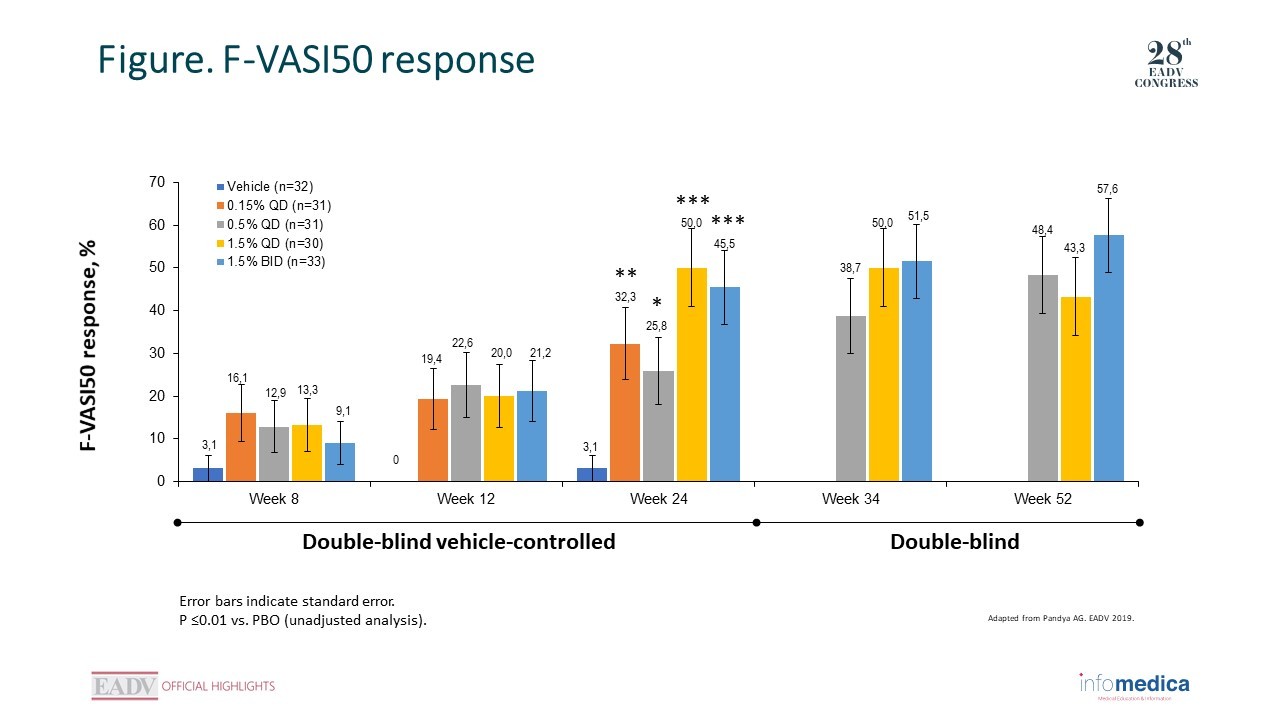
The primary endpoint was proportion of patients treated with ruxolitinib cream who achieved a ≥50% improvement from baseline in F-VASI (F-VASI50) at week 24 compared with patients treated with vehicle.
At week 24, F-VASI50 was achieved by a significantly greater proportion of patients receiving ruxolitinib cream (25.8%–50.0% across doses) vs vehicle (3.1%).
At week 52, the proportion of patients achieving an F-VASI50 response was highest in the 1.5% BID group (Figure).
At week 52, the proportions of patients achieving F-VASI75 and F-VASI90 responses were highest in the 1.5% BID group.
T-VASI50 at week 52 was achieved by patients in a dose-dependent manner.
Among patients who treated all depigmented skin (baseline total BSA ≤20%), T-VASI50 response was 45.0% with the 1.5% BID regimen at week 52.
The proportion of patients who attained Physician's Global Vitiligo Assessment (F-PhGVA) scores of clear or almost clear at week 24 increased by week 52.
Ruxolitinib cream was not associated with clinically significant application site reactions or serious treatment-related adverse events.
Most relevant TEAEs include acne and possible application site reactions.
Ruxolitinib cream monotherapy produced substantial facial and total body repigmentation of vitiligo lesions after week 24.
Continued improvement was seen through 52 weeks of treatment (highest responses with 1.5% BID), suggesting that ruxolitinib cream is an effective treatment option for patients with vitiligo.
A longer duration of therapy was associated with greater repigmentation, objectively assessed using the VASI.
Near-complete facial repigmentation as assessed by F-VASI75.
Substantial total body repigmentation as assessed by T-VASI50.
All doses of ruxolitinib cream were well tolerated, and no treatment-related serious AEs were reported.
Key messages/Clinical perspectives
Ruxolitinib cream monotherapy appears to be a promising therapy for vitiligo lesions with good long-term durability.
Rashighi M, Harris JE. Interfering with the IFN-γ/CXCL10 pathway to develop new targeted treatments for vitiligo. Ann Transl Med. 2015;3(21):343.
Quintás-Cardama A, Vaddi K, Liu P, et al. Preclinical characterization of the selective JAK1/2 inhibitor INCB018424: therapeutic implications for the treatment of myeloproliferative neoplasms. Blood. 2010;115(15):3109-17.
Rosmarin D, et al. Efficacy and safety of ruxolitinib cream for the treatment of vitiligo: results of a 24-week, randomized, double-blind, dose-ranging, vehicle-controlled study. Presented at: World Congress of Dermatology 2019.
Presented by: Prof. Kristian Reich, Translational Research in Inflammatory Skin Diseases, Institute for Health Services Research in Dermatology and Nursing, University Medical Center Hamburg-Eppendorf, and Skinflammation® Center, Hamburg, Germany
Presented by: Prof. Spyridon Gkalpakiotis, Department of Dermatovenereology, Third Faculty of Medicine and University Hospital of Kralovske Vinohrady, Prague, Czech Republic.
 RATE THIS PROGRAM
RATE THIS PROGRAM

 Deutsch
Deutsch Español
Español Français
Français Italiano
Italiano Português
Português יהודי
יהודי